Airborne Infections
Aerosol Transmission of Respiratory Infections
Aerosol Transmission of Respiratory Infections
Introduction
Respiratory infections can be transmitted through three main modes: touching pathogens directly; splashes and sprays of drops that land on the eyes, nose, or mouth; and inhalation of aerosols. Although “airborne transmission” is a more general term that could refer to transmission by splashes and sprays or by aerosols, it is often used in reference to aerosol transmission. Although the relative importance of the various transmission modes is uncertain for various respiratory viruses and bacteria, this third transmission mode – via inhalation of infectious aerosols – has been implicated by epidemiologic and experimental studies as a likely driver of the population spread of influenza, measles, chickenpox, SARS, and other respiratory infections.
The main findings of related scientific research are as follows:
Overview of Aerosol Transmission
Critical Scales and Settings
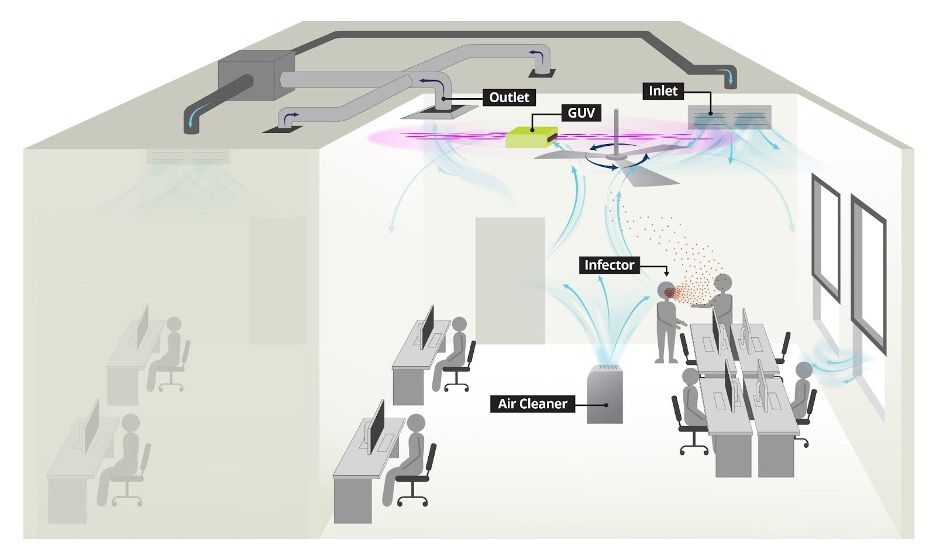
The application and assessment of infectious aerosol controls indoors can be considered at three transfer scales: a) close-interactive, b) room, and c) building (between-room). Administrative controls for all scales of transfer include pre-entry screening, face mask or respirator use as source control and PPE, activity limits (e.g., restricted loud speech, singing, or exercising), and frequent cleaning of common touch surfaces.
Overview of Indoor Environment Controls Against Airborne Infection
Exposure at room scale is important because of the potential for high concentrations of infectious aerosols, large numbers of exposed individuals, and prolonged exposure durations. Superspreading has been well-documented at this scale, and controls effective at this scale have the greatest potential to mitigate exposures and outbreaks at the community level.
Indoor Environment Control Strategies to Reduce Aerosol Transmission
Building Ventilation
Ventilation in buildings is defined as the rate at which outdoor air flows into an indoor environment and replaces the existing air. Mechanical ventilation uses fans to draw air into an indoor environment, while natural ventilation includes air flow from infiltration through the building envelope and from the opening of windows or doors. Because it is understood that infected humans can generate infectious aerosols that can float through indoor environments leading to inhalation exposure by others sharing the indoor air, ventilation offers to reduce the concentration of infectious aerosols – through dilution and removal – that might otherwise accumulate.
Aerosol Filtration
Filtration systems can reduce pathogenic airborne particle concentrations, reducing exposure and potentially reducing infection risk and/or severity of illness. Potentially infectious aerosols generated from the respiratory tract are typically 1-10 µm, and generally have a lower bound of 0.5 µm.
Air Disinfection
Germicidal ultraviolet irradiation (GUV, sometimes abbreviated UVGI) has been used to successfully control airborne infection since the 1930’s. It produces short wavelength light (or irradiance) within the 200-280nm spectrum of UVC, which interferes with the genetic material in viruses, bacteria, molds, and other organisms, thus, rendering them noninfectious.
Air Flow and Distribution
It is known that infectious aerosols travel through the air on prevailing air currents after generation from infected humans. Air flow dynamics can influence infectious aerosol exposure. Air flow influences the aerosol control efficacy of building-level ventilation, filtration, and germicidal UV systems. It also influences outdoor exposure to potentially infectious aerosols.
Resources to Estimate Risk
Tools for estimating exposure or risk for SARS-CoV-2 in indoor environments; summary documents and helpful resources.